Cancers of the large intestine
Symptoms and causes
Symptoms and causes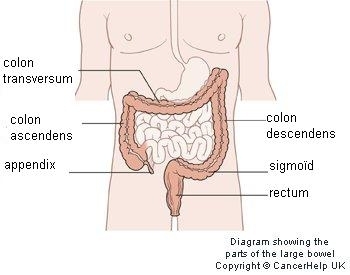
What is cancer of the large intestine?
The large intenstine consists of:
- the colon: with an ascending portion (colontype ascendens), transverse portion (colon transversum), descending portion (colon descendens) and sigmoid colon.
- the rectum
- the sphincter (anus)
The large intestine is part of the digestive tract: food is digested in the large intestine; water and other substances are taken in and then exchanged with blood. Undigestible parts and waste products are disposed of.
Colon cancer almost always develops as an intestinal polyp. A polyp (adenoma) is a protrusion or a thickening of the muscoa that lines the inside of the intestine. Polyps are benign tumours, but some of them can grow into malignant tumours. Most colon tumours are made from glandular cells (adenocarcinoma). Within the group of large intestine cancers, there are:
- colon tumours, where there is a tumour located in the colon ascendens, colon transversum, colon descendens or the sigmoid
- rectal tumours, where the tumour is less located less than then 15-cm anus
Each type requires a slightly different approach to treatment.
Symptoms
You cannot feel cancer of the large intestine. A small amount of blood with bowel movements or abdominal cramps are not a reliable sign of large intestine cancers. Such symptoms may be caused by a number of other conditions.
Anal bleeding that is red can also be from various causes, but the presence of a malignant intestinal tumour is one of the most important ones. Uncontrolled weight loss is certainly another reason for worry. If you have abdominal cramps together with weight loss and/or anal bleeding, you should schedule a large intestine examination - and especially if the symptoms persis and/or if you are older.
Changes in your bowel moment pattern (less frequent or more frequest bowel movements) and persistent diarrhoea or constipation (in spite of medication) may also be signs of a large intestine cancer.
Diagnosis and treatment
Diagnosis and treatment
Clinical studies
How is the diagnosis made?
The classic colonoscopy is the most widely-used detection method because not only is it highly accurate, but also because any susicious tissue found during the examination (e.g. biopsies or polyps) can also be removed during the test. The pathologist analyses the pieces of suspicious tissue under the microscope. This takes approximately three working days.
Cancer of the large intestine is also looked for recently using stool tests.
Staging
Usually, there is a gradual growth with damage to part of the intestinal wall and then the entire wall. When cancer cells become detached from the original tumour and penetrate deep enough to reach the blood and lymph vessels, they can escape and colonise glands. If a detached clump of cancer cells nest within another part of the body, the cancer is said to have spread or ‘metastasised’. Large intestine cancer cells sometimes end up in the liver or lungs. The stage is determined according to a global system: the Tumour Node Metastasis (TNM) classification system. This looks to see whether the tumour has grown through the intestinal wall (T), and if the lymph nodes have been affected (N) and when whether they have metastasised (M).
Treatment
The most common treatment for cancer of the large instestine consist of oncological surgery, radiation therapy, chemotherapy and targeted therapy.
The attending physician may ask a patient to participate in scientific research (also called a clinical study or trial). For patients, participation in a study often represents an additional treatment option. In clinical trials, physicians test whether a new drug or treatment is safe and produces better results than existing treatments. However, a patient will only participate if he or she gives his or her express consent.
For more information, please go to the website for the Digestive Centre
Treatment centres and specialisations
Treatment centres and specialisations


Latest publication date: 24/01/2024
Supervising author: Dr Monsaert Els